
Your brain is 2% of your body weight and holds nearly a quarter of your body’s total cholesterol. Driving that number toward the floor has consequences — and the data on mood, cognition, and statin side effects in active people is some of the most under-discussed evidence in modern medicine.
The first post in this series walked through how to read a lipid panel correctly. The second showed you what the largest mortality studies in the world actually reveal about cholesterol and longevity. This is the post that ties the biology together.
Because the deeper question — beyond “does lower cholesterol mean longer life?” — is what does cholesterol actually do in the body, and what happens when we drive it toward levels we were never designed to maintain?
The answer starts in the organ that holds the most cholesterol of any tissue in the body. Your brain.
What cholesterol is actually doing up there
Open any neurology textbook and you’ll find the same fact: cholesterol is one of the most abundant molecules in the central nervous system. The brain accounts for about 2% of body weight and contains 23-25% of the body’s total cholesterol. Cholesterol concentration in brain tissue is 15-30 mg per gram, while the average in other tissues is 2-3 mg per gram. The brain is, biochemically, a cholesterol-built organ.
This is not architectural decoration. Cholesterol’s functions in the brain include:
Building myelin. Myelin is the insulating sheath that wraps around nerve fibers and allows electrical signals to propagate quickly along axons. Myelin dry weight is roughly 70% lipid, 30% protein — the inverse of most cell membranes. Cholesterol is one of the three major lipid components of myelin, present at approximately 40 mg per gram with a half-life of about five years. Without adequate cholesterol availability during development and throughout life, myelin formation is compromised. Demyelinating diseases — multiple sclerosis, leukodystrophies — are conditions of failed myelin maintenance.
Forming synapses and dendrites. Synapses are the connection points between neurons. Cholesterol is required for synapse and dendrite formation, for axonal guidance during development, and for the membrane structure that allows neurotransmitter release. Research has demonstrated that cholesterol depletion in neurons impairs synaptic vesicle exocytosis, neuronal activity, and neurotransmission, leading to dendritic spine and synapse degeneration.
Generating neurosteroids. The brain manufactures its own steroid hormones — pregnenolone, allopregnanolone, dehydroepiandrosterone (DHEA) and others — that act locally on neurons to regulate mood, cognition, anxiety, and stress response. The starting molecule for every one of these neurosteroids is cholesterol.
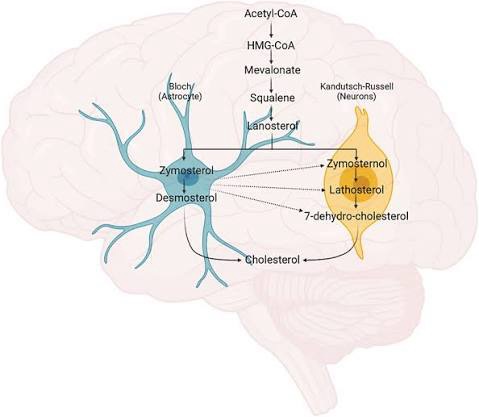
Here is where the honest caveat lands. The blood-brain barrier prevents lipoprotein-bound cholesterol from crossing freely into the brain. More than 95% of brain cholesterol is synthesized locally, primarily in glial cells called astrocytes. This means dietary cholesterol does not “feed the brain” in the simple way some health writers have framed it.
But — and this is the part that matters — the brain’s cholesterol production uses the same biosynthetic enzymes as the rest of the body. Statins inhibit HMG-CoA reductase, the rate-limiting enzyme of cholesterol synthesis, systemically. They cross the blood-brain barrier (some more than others). They reduce cholesterol synthesis everywhere, including in the brain. The peripheral cholesterol economy and the brain cholesterol economy are not two separate systems. They are two outputs of the same machinery.
And outside the brain, cholesterol’s role is just as foundational. It is the substrate for every steroid hormone in the body. Cholesterol becomes pregnenolone, which becomes progesterone, cortisol, aldosterone, DHEA, testosterone, and estradiol. It is also the substrate for vitamin D synthesis — UV radiation converts 7-dehydrocholesterol in the skin into vitamin D3. Drive systemic cholesterol too low and you compromise the substrate pool for hormone production, vitamin D synthesis, and the membrane composition of every cell in the body.
This is not a “cholesterol is good” oversimplification. It’s a recognition that cholesterol is a foundational structural and signaling molecule. Treating it as a pathogen to be eliminated reflects a misunderstanding of basic biochemistry.
The depression and suicide data
When researchers have looked at serum cholesterol in populations with mood disorders, the pattern is consistent and striking.
A 2020 meta-analysis published in PLOS One combined 32 studies involving 7,068 participants with major depressive disorder. The result: patients who had attempted suicide had significantly lower serum concentrations of total cholesterol (standardized mean difference -0.63) and low-density lipoprotein cholesterol (SMD -0.69) compared to non-attempters. The proposed mechanism is that low cholesterol concentrations alter brain cell membrane fluidity in ways that impair serotonin binding and signaling.
A larger meta-analysis published in the Journal of Psychiatry and Neuroscience combined 65 studies covering 510,392 participants. The authors concluded that low serum lipid levels are a predictive marker not only for completed suicides, but for suicidal ideation, suicide attempts, and suicidal tendencies. The pattern held across diverse populations and study designs.
University of Minnesota researchers found that people with total cholesterol below 160 mg/dL had higher suicide rates than those with higher cholesterol levels. Swedish researchers comparing cholesterol measurements of nearly 80,000 men and women against subsequent arrests for violent crime found that low cholesterol was associated with increased risk of criminal violence — a finding replicated across multiple populations.
The mechanism that ties these findings together is membrane biology. Serotonin receptors sit in cell membranes whose composition includes cholesterol. When cholesterol drops, membrane fluidity changes, and receptor function is altered. This is not a fringe hypothesis. It’s documented in basic neurochemistry research and reproduced across study after study.
This does not mean that everyone with low cholesterol becomes depressed or violent. It means the correlation is real, the mechanism is plausible, and the implication is one that mainstream cholesterol guidelines do not address: pushing serum cholesterol below a certain threshold has documented neuropsychiatric costs.
The dementia picture is messier — and the truth is in the messiness
This is where the honest accounting matters. The data on cholesterol and dementia does not all point in one direction. Some studies find that higher LDL in mid-life is associated with greater Alzheimer’s risk later. Others find the opposite. A 2025 South Korean study of over 570,000 people found that LDL levels below 70 mg/dL were associated with a 26% reduction in all-cause dementia risk — but importantly, when LDL fell below 30 mg/dL, the protective effect disappeared. Below a certain threshold, lower stopped being better.
A separate large study published in 2024 found that cholesterol variability — how much someone’s cholesterol fluctuates year to year — was a stronger predictor of dementia risk than absolute cholesterol level. People with the greatest variability had a 60% higher dementia risk and a 23% higher risk of cognitive decline compared to those with the most stable cholesterol levels. The implication: stability matters as much as level, and the pattern of statin starts, stops, dose changes, and discontinuations that characterizes real-world statin use may itself be contributing to risk.
A systematic review of LDL and Alzheimer’s found that elevated LDL above 121 mg/dL was a potential risk factor for Alzheimer’s in the 60-70 age group, but the association vanished with advancing age. In other words: mid-life lipid patterns may matter for late-life brain health, but by the time someone is in their late 70s or 80s, the connection between LDL and dementia has functionally disappeared.
The honest takeaway is that we don’t yet have a single clean answer on cholesterol and dementia. But the U-curve pattern shows up here too — too low is associated with cognitive risk, very stable mid-range levels appear protective, and the relationship shifts with age.
Anyone who tells you the dementia data is simple is selling you something.
What statins actually do to active people
If you exercise — and especially if you train hard — the statin conversation is fundamentally different from the one your doctor is having with their sedentary patients. The published incidence of statin-associated muscle symptoms in the general population is 1-10% depending on the source. In active populations, the reported incidence runs as high as 75%.
That number is not a typo. A clinical research program at the University of Copenhagen tracking statin users found that the reported incidence of myalgia ranged from 1% in pharmaceutical company reports to as high as 75% in statin-treated athletes. The mechanism appears to be statin-induced impairment of muscle mitochondrial function, particularly through depletion of coenzyme Q10 — a critical cofactor in the mitochondrial electron transport chain that is produced through the same metabolic pathway statins block.
This matters in two ways.
First, it directly degrades training response. Statin-induced mitochondrial dysfunction reduces aerobic capacity, slows recovery, and impairs muscle protein synthesis signaling. Active people on statins report measurable decreases in time to exhaustion, peak power output, and exercise tolerance. The same exercise that produces a robust training adaptation in someone off statins produces a blunted response in someone on them.
Second, it directly contradicts the primary prevention rationale. Statins are prescribed in part to reduce cardiovascular risk, and exercise is one of the most powerful interventions for reducing cardiovascular risk. If the statin causes the muscle pain that causes the patient to exercise less, the medication is undermining the lifestyle factor that would have produced larger cardiovascular benefits than the medication itself.
The number-needed-to-treat math for statins in primary prevention is also worth understanding. A Cochrane review analysis showed that for every 200 patients without established cardiovascular disease who take statins daily for five years, one death is prevented. That is the actual benefit, in the population that is being prescribed statins most aggressively. The trial data does not show massive mortality reductions in primary prevention. It shows modest, statistically detectable reductions in a tiny fraction of users — at the cost of muscle pain in a large fraction, increased risk of new-onset type 2 diabetes in a documented subset, and the cognitive complaints that some statin users report and that the published literature debates without resolving.
This is not an argument against statins for everyone. There are patient populations — familial hypercholesterolemia, established cardiovascular disease, very high ApoB combined with elevated Lp(a) and inflammation — where the risk-benefit calculation favors treatment. The argument is against the casual, unconditional, “your cholesterol is 240, start on this and we’ll recheck in three months” prescribing that defines current primary care practice.
For active people, the conversation has to include the muscle, mitochondrial, and exercise-capacity costs. Most of the time, it doesn’t.
What this series has been about
Three posts, one argument.
Post 1 showed you how to read a lipid panel — including my own — and how the standard three or four numbers everyone is taught to fear are nearly useless without the markers that contextualize them. Trig/HDL ratio, hsCRP, fasting glucose, and HDL itself tell you more about cardiovascular risk than total cholesterol and LDL do, and ApoB plus a CAC scan effectively closes the case for the people willing to ask for them.
Post 2 showed you the longevity data — the Korean 12.8 million person study, the Honolulu Heart Program, the HUNT 2 Norwegian cohort, the Sardinian Blue Zone nonagenarians. The mortality nadir for total cholesterol in older adults is not under 200 mg/dL. It sits between 210 and 249. For women specifically, the relationship between cholesterol and mortality is inverse. “Lower is always better” is not what the data shows.
This post addressed the biology that makes the longevity data make sense. Cholesterol is a structural and signaling molecule. The brain is built out of it. Hormone production depends on it. Membrane function depends on it. Driving it toward the floor with pharmaceuticals has documented effects on mood, neurocognitive function, and — for active people specifically — muscle function and exercise capacity. None of these costs make it into the patient conversation when a prescription is written.
The result of all of this — across the whole series — is not “ignore your cholesterol.” It’s learn what your panel actually means before agreeing to a treatment plan. Calculate your trig/HDL. Demand an hsCRP. Ask about ApoB. Consider a CAC scan after 40. Understand that the framework you’ve been taught was built on incomplete data, conservative interpretations of conflicting trials, and three decades of commercial pressure pushing in one direction.
The people who walk into their physicals already understanding this don’t walk out with prescriptions they didn’t need. They walk out with answers, real risk assessments, and the agency to make decisions about their own health. That’s the version of the cholesterol conversation everyone deserves, and almost nobody is getting.
If you’re already on a statin and reading this, please do not stop your medication based on a blog post. Bring this framework to your next appointment, ask for the markers we’ve discussed, and have an actual conversation with your doctor about what your full risk picture looks like — not just one or two numbers in isolation. Some people genuinely need the medication. Many do not. The only way to know which category you’re in is to see the whole panel through a properly informed lens.
That’s the work.
This is the final post in the three-part cholesterol series.
- My Doctor Would Tell Me to Take a Statin. Here’s Why They’d Be Wrong.
- The Cholesterol Longevity Data Your Doctor Won’t Show You.
- Your Brain on Low Cholesterol: The Statin Conversation Nobody’s Having. (this post)
